The Top Five Complaints
Prosthodontics – what could go wrong?
Indirect restorations are commonly associated with longevity1,2 and most dentists would know that the literature supports a success rate for conventional crowns of at least 90% at ten years.3 Similarly, the survival rates of implant-supported single crowns and implant-supported bridgework are reportedly high. The results from independent Scientific reviews, coupled with direct clinical observation, inspires confidence in clinicians and crowns remain the treatment of choice when it is necessary to protect the integrity of heavily broken down, endodontically-treated or traumatised teeth.
Over time, developments in materials and techniques have resulted in restorations with better strength and improved aesthetics4. Clinicians are also able to deliver indirect restorations via a more streamlined workflow.5 So, why are prosthodontic services in general and crowns/bridgework in particular one of the most complained about treatment modalities in SA? This article will explore three areas of complaint identified and reported to ADA SA during a twelve-month period. As members of the ADA, you have access to online lectures and webinars via the ADA digital media library and to journal articles via the ADA National Library. If you are interested in learning more, ADA SA will be running a series of face-to-face courses in Adelaide during 2024 to explore ways of avoiding and managing procedural mishaps – we hope to see you there!
Common problems:
- Patient-identified problems: aesthetics, de-bonding, fracture
Debonded crown at 6 months
The most commonly-reported issue relating to indirect restorations (apart from cosmetic dissatisfaction) is early failure ie: the crown or prosthesis requires replacement in the first 24 months. Patients are never happy when their new crown falls off or breaks particularly when they feel they have invested time and money to achieve a high-quality and lasting outcome. Factors which may contribute to the early debonding of a crown include faulty restoration planning or tooth preparation technique, improper bonding/cementation techniques, incorrect selection of cement, improper preparation of surfaces, inadequate isolation/moisture control, or failure to follow manufacturers instructions regarding cementation. It is worthwhile noting the ADA Schedule and Third party committee describes the fundamental characteristic of a complete crown is that the restoration by design has adequate retention and resistance form.

Catastrophic fracture
Early catastrophic fracture of a bonded crown could be due to occlusal factors, poor handling of material in the lab, excessive adjustments chairside without coolant causing crack propagation, improper bonding of ceramics leaving the crown unsupported and/or poor design of tooth restoration, poor tooth preparation or materials selection.
Whatever the cause, early failure of indirect restorations is often emotionally fraught due to the cost of the restoration which is often compounded by initial high patient expectations. Coupled with this initial dismay, might be a loss of confidence in the dentist who performed the treatment with the patient often seeking a second opinion from an alternate clinician. All too often, this combination leads to unhappy patients complaining about their dentist.
- Clinician-identified problems: margins, contacts, overhangs, excess cement, radiolucencies
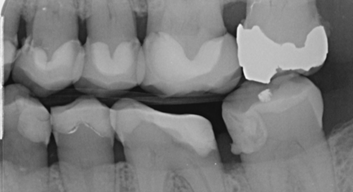
Marginal defects and overhangs
Whilst the patient is often the first to know if their new crown is not aesthetically pleasing or when it fractures or falls off, there can be other, more occult issues which may not be evident to the patient but which are readily identifiable by an examining clinician. Such problems include marginal defects, overhangs, extruded cement, inadequate margins or open contact areas. The discovery of any one of these issues soon after crown cementation can be unsettling for the treating practitioner (particularly for less experienced clinicians). However, once you have identified an issue, your duty of care to the patient requires the situation to be explained and a remedy suggested. Such problems should never be overlooked and identifying an issue should be regarded as an opportunity for rectification. Unresolved issues are almost always going to escalate with the passage of time and, if they problem is identified by another clinician or practice, can result in an angry letter of demand.
It is always best to identify and treat issues early on with comprehensive records being obtained at each step of the process. It is also recommended that a post-cementation image is obtained. This will enable you to confirm that:
- The crown is fully seated
- The periodontal condition/bone support is satisfactory
- There is an absence of radiolucencies
- The contact areas are satisfactory
Your comprehensive records are your best defence that the completed restoration was ideally placed at cementation if an issue should arise down the track. For the longevity of your restoration to be assured, your patient must not only understand but also be able to carry out the maintenance requirements needed.7 Finally, it is important to provide the patient with a realistic estimate regarding the expected longevity of the restoration. As a guide, the expected longevity of a crown restoration would generally be 7-10 years. Some patients unfortunately form an opinion that their restorations will last forever and once they are convinced of this, it can be difficult to advise them otherwise. The ADA has developed clinical resources such as information sheets (ADA Patient Education Pamphlets for Dentists | Mi-tec Medical Publishing (mitec.com.au)) and (free) online resources ( Crowns, bridges and veneers - Australian Dental Association (teeth.org.au)) to assist with patient education and help you to manage expectations.
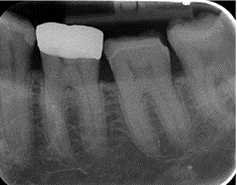
- Post-operative complications – pain or discomfort
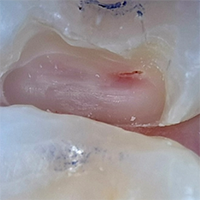
Large pulp horn with exposure
Initial and minor post-operative discomfort is not unusual following crown insertion as the gingival tissues recover and the restoration settles into the occlusion. Significant and prolonged problems, however, should be investigated and may relate to tight contacts, excess cement, violation of the biological width, an occlusal interference or an endodontic problem. To avoid such sequelae, as part of your pre-operative assessment, it is important to perform an occlusal and endodontic assessment of the tooth – making sure to perform vitality testing and take an IOPA radiograph which clearly shows all root apices and surrounding bone. If the pulp status is in question, or if the tooth has recently been restored, consider delaying construction of the prosthesis or, alternately, employing a long-term provisional restoration. Even with a healthy pulp, there is a chance of pulpal involvement after crown preparation so clinicians should still warn their patients that this could be a potential complication that can occur in future as a result of the treatment. If there is an existing RCT, always consider specialist assessment and/or replacement prior to making the crown. If the tooth has been endodontically treated, consider when and if to place a post and what types of post/cores are suitable to achieve optimal clinical outcomes. Liaising with your treating specialist endodontist can help successful planning/execution of the post/core.
Managing problems
If an adverse outcome occurs, communicate with the patient regarding all options to address it. If managing the situation is out of your scope, refer to an appropriate practitioner. You should address any financial aspects as soon as practicable – including the extent to which additional fees or charges might apply. Your willingness to explain the situation and support the patient through the rectification journey may well prevent a regulatory or civil complaint being made against you. If you are unsure what to do, call your ADA Peer advisor for a confidential discussion. Remember, most procedural mishaps (which cannot be managed immediately and effectively by the treating practitioner) are notifiable events. You should report any such occurrences to you PII provider and seek assistance, support and advice.
*Cited references are available upon request
**ADA SA acknowledges and thanks Dr Amal Ibrahim for her expertise and assistance in the preparation of this article.
Dr Jane Pinchback, Peer Advisor, ADA SA